
Cholesterol 101: Everything You Need to Know (And Then Some!)
Are You Confused About Cholesterol? You’re Not Alone!
Cholesterol has become one of the most polarising—and misunderstood—topics in modern health.
Depending on where you look, dietary fat is either the primary driver of disease or completely irrelevant.
Eggs are demonised in one headline and celebrated in the next.
Low-fat, low-carb, Mediterranean, ketogenic—it’s easy to lose sight of what actually matters.
But here’s the reality: cardiovascular disease remains one of the leading causes of death worldwide. And despite all the noise, the science is actually quite consistent.
Even better? The most powerful tools to improve your cholesterol—and your long-term health—are completely within your control.
Let’s break it down clearly.
Cholesterol Isn’t Just About Your Heart
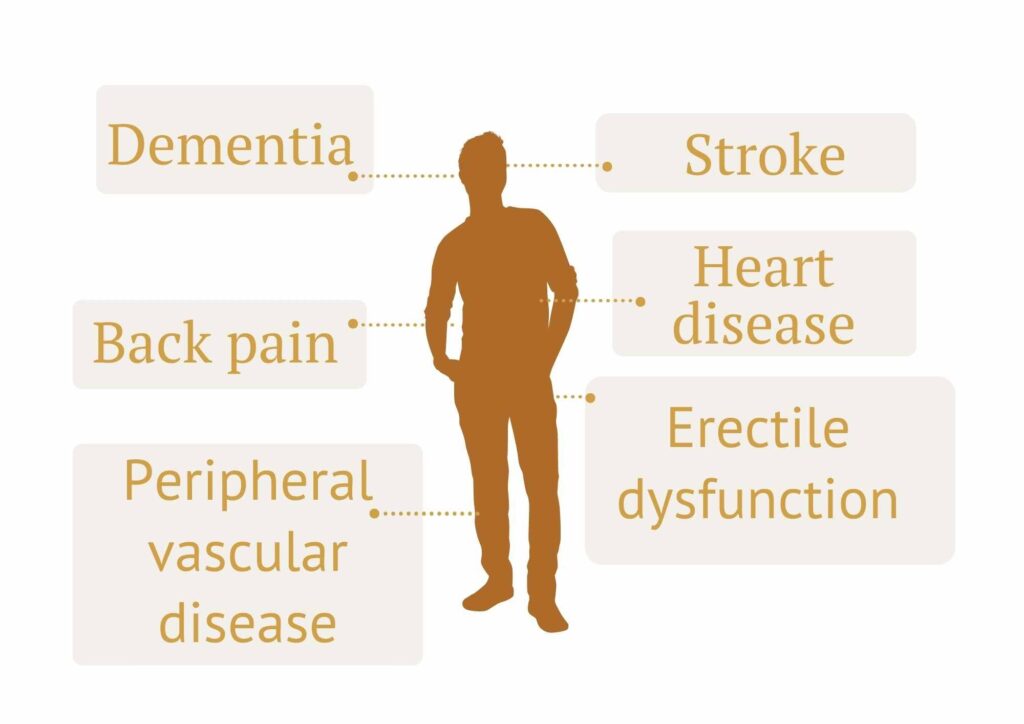
Most people think cholesterol = heart disease.
But that’s only part of the story.
The same process that leads to heart attacks can also affect:
- the brain (increasing risk of stroke and memory decline)
- blood flow to the legs (peripheral vascular disease)
- sexual function (causing erectile dysfunction)
- even things like chronic back pain over time
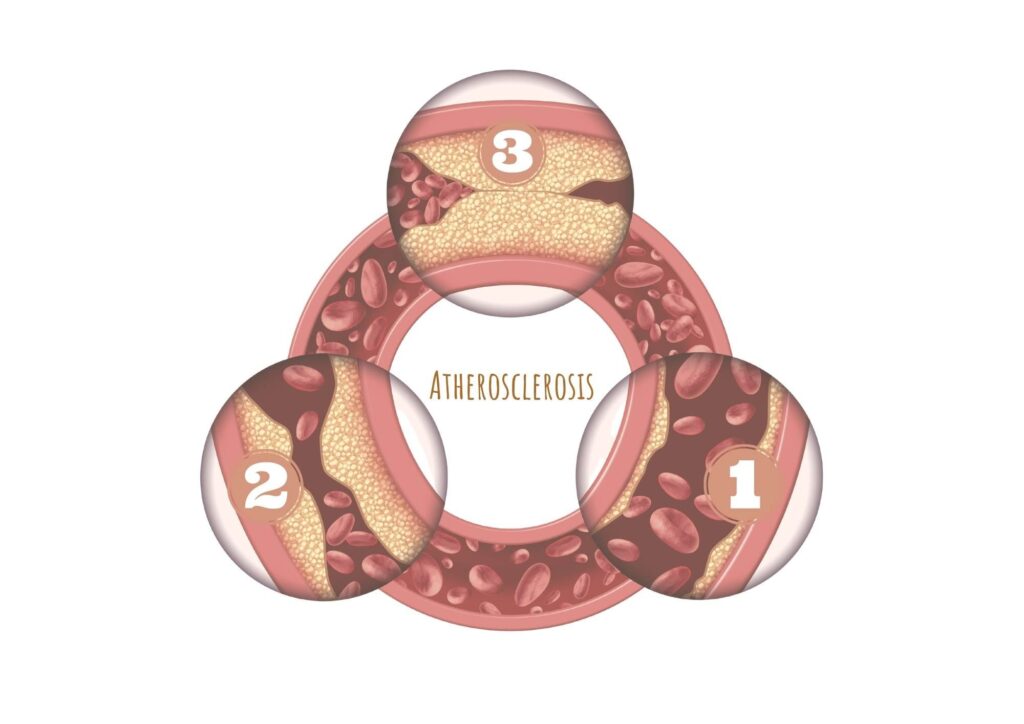
What ties all of this together is a slow build-up of plaque in the arteries—known as atherosclerosis.
It’s not just a “heart problem.” It’s a whole-body issue that develops quietly over many years.
Genetics Play a Role—But They Don’t Decide Your Fate
You’ve probably heard that high cholesterol “runs in families.”
That’s true to a degree. Genetics can influence your risk, and are estimated to account for around 40–60% of coronary artery disease risk
But here’s the important part:
Even if high cholesterol runs in your family, your daily habits still make a huge difference.
In fact research shows that people with high genetic cholesterol levels can cut their chances of heart disease nearly in half just by improving lifestyle factors.
So yes—genes matter.
But they’re not the whole story.
This Process Starts Earlier Than Most People Think
Atherosclerosis is not a disease of old age.
It’s a lifelong process.
Early changes can begin forming in childhood, and atherosclerotic plaques are often present by early adulthood – sometimes as soon as your 20s!
Clinical events (heart attacks, strokes) are simply the late-stage consequence that show up decades later.
This is why updated 2026 AHA guidelines now emphasize earlier detection and earlier intervention:
- Routine cholesterol screening recommended from age 19
- Cholesterol levels should be checked every 5 years from this age onwards (or more often if risk factors are present)
- Earlier testing (ages 9–11, or even from age 2) should be considered if there’s a very strong family history of early heart disease or severe high cholesterol.
The focus now is simple:
Lower your exposure over the long term, rather than just patching up the damage later.
Because prevention is powerful – and it starts early.
Why Cholesterol Isn’t Always The Problem
This is where things often get misunderstood.
Cholesterol is a waxy substance in your blood, but it isn’t inherently “bad.”
Your body actually needs it to:
- Build cell membranes
- Produce hormones
- Make vitamin D
- Help digest fats via bile acid formation
The real issue is how cholesterol is transported in your blood—and where it ends up.
Think of it like this:
- If it stays in the bloodstream and is properly managed → no problem
- If it gets stuck in artery walls → that’s when trouble starts
But did you know, your liver makes all the cholesterol you need. You don’t actually need to get it from food!
And cholesterol is only found in animal products.
This is why people who follow plant-based diets tend to have much lower cholesterol levels overall, along with lower rates of cholesterol-related health problems (and why whole food plant focused diets are recommended for better heart and brain health).
We’ll talk more about how different foods affect cholesterol levels in just a moment, but first, let’s take a look at what makes cholesterol “good” or “bad.”

It’s Not Just ‘Good’ Or ‘Bad’ Cholesterol Anymore
If you’ve had a cholesterol test, you’ve probably heard of “good” (HDL) and “bad” (LDL) cholesterol.
These refer to high density lipoprotein (HDL) and low density lipoprotein (LDL) – particles that transport cholesterol around your body.
These are still useful markers—but they miss some vital parts of the puzzle.
More recent research has started to focus on how many harmful particles (re recent guidelines are shifting the focus more towards “atherogenic lipoproteins”) are actually circulating in your blood, not just how much cholesterol they carry.
These are small dense particles that can get into your artery wall and contribute to plaque formation.
They include:
- LDL
- VLDL and remnant particles
- Lipoprotein(a)
- Other ApoB-containing particles
Confused yet?
Let’s break this down further:
HDL: The Good Guy
HDL stands for high density lipoproteins. These are particles that remove cholesterol from your arteries, and send it back to the liver where it can be used
HDL is ‘good’, because higher levels = more protection for your heart and blood vessels
ApoB: The Number That Often Tells the Real Story
Here’s where it gets more interesting.
Every harmful cholesterol particle in your blood carries one molecule of a molecule you’ve probably never heard of – apolipoprotein B (ApoB).
So instead of just measuring how much cholesterol is in your blood, ApoB tells you how many atherogenic particles are actually capable of causing damage
Why does this matter?
Because two people can have the same LDL level—but very different numbers of particles, and therefore very different risk.
It’s particularly relevant in people who’s cardiovascular risk may be underestimated by checking LDL alone – such as those with high triglycerides, insulin resistance, and metabolic dysfunction.
This is why the 2026 lipid guidelines now recommend ApoB testing in specific situations to refine risk and guide treatment, particularly in those with:
- Diabetes
- High triglycerides
- Metabolic syndrome
- Patients who have reached LDL targets but may still have residual risk
In these cases, ApoB is often a more accurate predictor of cardiovascular risk than LDL alone.
The bottom line: you can have a “normal” LDL—but still be at high risk if your ApoB is elevated.
This is one of the key reasons the guidelines are no longer just about cholesterol—they’re about lipoprotein biology.
Lipoprotein(a): The Genetic Risk Factor Most People Miss
Another important piece of the puzzle is Lipoprotein(a), often shortened to Lp(a).
This is something you’re born with—it’s largely genetic – meaning that unlike other markers, you can’t change it much with diet or lifestyle.
But it still matters. A lot.
High Lp(a) levels can:
- speed up plaque build-up significantly
- increase inflammation levels and cardiovascular risk
- raise clotting risk
Lp(a) can help explain “unexpected” heart disease in otherwise healthy people.
That’s why newer guidelines recommend checking it at least once in your life.
If it’s high, it doesn’t mean something is “wrong”—but it does mean you may need to be more proactive with other risk factors.
In other words, Lp(a) helps identify people who need to be treated more intensively—even if their standard cholesterol tests looks ok.
LDL Still Matters (A Lot)
Even with all these newer markers, one thing hasn’t changed:
LDL is still important.
LDL is known traditionally as the ‘bad cholesterol’; it stands for low density lipoproteins.
These are small dense particles which are able to get inside your artery walls and deposit cholesterol there, which drives plaque (atherosclerosis) formation
Despite what you might have heard, higher levels of LDL still = higher risk of heart disease
In fact there’s decades of cumulative evidence that lowering LDL will reduce your cardiovascular risk.
In fact, studies show that for every 1% you reduce your LDL cholesterol, you reduce your relative risk of heart disease by up to 23%.
The main update in the 2026 lipid guidelines, is that there are now clearer LDL targets to aim for, depending on your risk level.
And the key idea is this:
It’s not just how high your LDL is—it’s how long your body is exposed to it.
Think of it like sun exposure.
A little over time is manageable.
A lot over decades adds up.
Don’t Forget Triglycerides
Triglycerides don’t get as much attention, but they’re incredibly useful, and another key piece of the puzzle.
Triglycerides are essentially your body’s way of storing excess energy.
High levels often point to:
- too much refined carbohydrate intake
- excess calories
- insulin resistance
- fatty liver
They’re less about cholesterol itself and more about how your body is handling energy.
They’re also closely linked to ApoB particle burden and cardiovascular risk.
As an added bonus, triglycerides can give you extra clues about your overall metabolic health – as your Triglyceride:HDL ratio is a helpful marker for insulin sensitivity (see below).

What Actually Happens In Your Body
This is the million dollar question – after all, why talk about cholesterol without understanding why it’s important.
As we mentioned earlier, the key is a process called atherosclerosis.
At a basic level, the process looks like this:
- Harmful particles enter the artery wall
- They become trapped and oxidized
- The immune system responds → inflammation
- Plaques form and grow over time
This process can unfold silently over decades before symptoms ever occur.
What Happens Next?
Once enough plaque builds up, things can go two ways:
- A sudden rupture → heart attack or stroke
- Slow narrowing → reduced blood flow over time
1. Plaque Rupture (Acute Events)
- Sudden clot formation
- Heart attack or stroke
2. Gradual Narrowing (Chronic Disease)
- Reduced blood flow
- Symptoms like angina, claudication, erectile dysfunction, back pain, or vascular dementia.
The Most Important Takeaway: This Is Largely Preventable
The 2026 lipid guidelines emphasize something that often gets lost:
Most cardiovascular disease is preventable
Lifestyle remains the foundation of treatment:
- Nutrition
- Physical activity
- Weight management
- Sleep
- Smoking cessation
Medication is layered on top when needed—not instead of these.

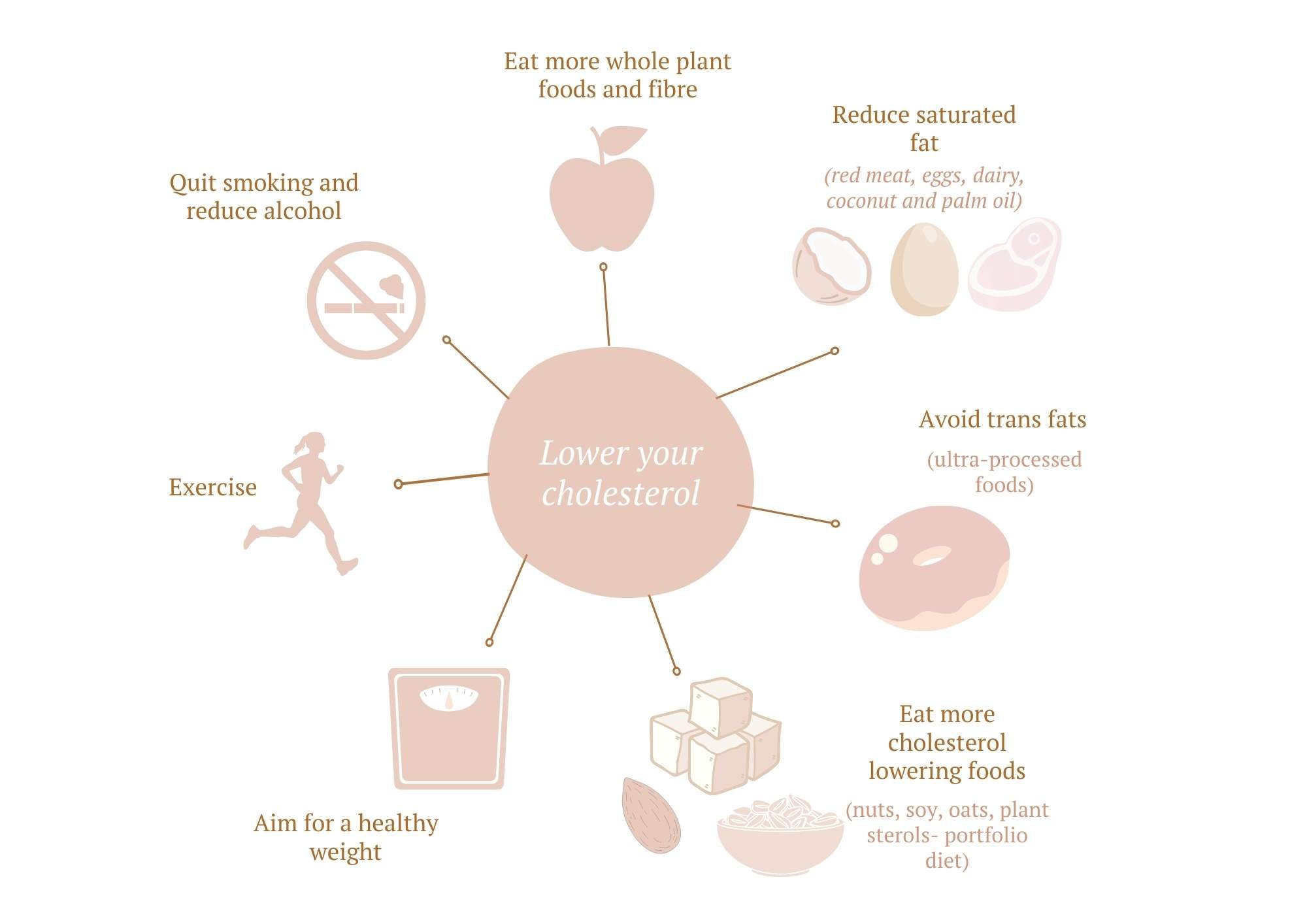
How Can You Improve Your Cholesterol Levels?
So now we’ve covered the basics of cholesterol, let’s dive into what you can do about it.
When you strip away the noise, the most effective interventions are remarkably consistent.
Diet
The strongest evidence supports:
- Whole, minimally processed foods
- High fiber intake
- Plant-predominant eating patterns
Two standout approaches include:
The Portfolio Diet
- Specifically targets LDL reduction
- Can reduce LDL by up to ~30% in controlled settings
The Mediterranean Diet
Emphasizes olive oil, nuts, legumes, whole grains, and vegetables
Strong evidence for cardiovascular event reduction
Eat To Reduce Your LDL
LDL levels are heavily influenced by the types of fats and cholesterol in your diet. The primary contributors are:
- Saturated fats.
- Trans fats.
- Dietary cholesterol.
As a general rule:
- Saturated fat → increases LDL
- Trans fats → increase LDL and inflammation
- Unsaturated fats → improve lipid profile
Fat Quality Matters More Than Fat Quantity
Saturated fat is the first piece of the puzzle, it’s found in:
- Fatty meats (e.g., red meat).
- Full-fat dairy products.
- Eggs.
Saturated fat increases LDL – for every 1% of your energy intake that comes from saturated fat, your LDL will increase by 0.02–0.04 mmol/L!!
This means the lower you can keep your saturated fat intake, the lower your LDL cholesterol will be.
Plants naturally contain little to no saturated fat (except tropical oils like coconut and palm oil), so shifting toward more whole plant foods and fewer animal products naturally lowers LDL cholesterol.
Dietary cholesterol comes next, foods high in cholesterol include:
- Egg yolks.
- Shrimp.
- Beef, pork, and poultry.
- Cheese and butter.
While dietary cholesterol raises LDL slightly, its effect is less significant than that of saturated fat.
Remember: Your body produces all the cholesterol it needs, so consuming dietary cholesterol isn’t necessary.
Trans fats are the third (and lesser known) piece of the LDL puzzles, these are artificially created fats found in:
- Processed foods (look for “partially hydrogenated oils” on labels).
- Small amounts in meat and dairy.
Trans fats increase LDL and decrease HDL, they’re also highly inflammatory and harmful for heart health – which is why they are banned in many countries, but can still sneak into many processed foods!
Key tip: Avoid trans fats entirely—they’re unnecessary and banned in many countries due to their link to heart disease.

STEPS YOU CAN TAKE TO LOWER YOUR LDL CHOLESTEROL
To lower your LDL cholesterol naturally, there are two main strategies you can use – reducing intake of foods that INCREASE LDL, and increase your intake of foods that REDUCE LDL.
REDUCE OR AVOID FOODS THAT INCREASE LDL:
- Avoid trans fats
- Limit saturated fats
- Choose healthy fats:
- Monounsaturated fats: Extra-virgin olive oil.
- Polyunsaturated fats: Non-tropical vegetable oils (e.g., sunflower, flaxseed).
- These fats can reduce LDL and increase HDL.
- Limit saturated fat intake to:
- <10% of your total calories.
- <7% if your cholesterol is already high.
BOOST YOUR INTAKE OF FOODS THAT REDUCE LDL:
In addition to avoiding foods that raise LDL cholesterol, you can actively reduce LDL levels by incorporating specific cholesterol-lowering foods into your diet.
One of the simplest and most effective steps is to increase your soluble fiber intake. Soluble fiber, found exclusively in plant-based foods, can significantly lower cholesterol levels. Incorporating fruits, vegetables, nuts, seeds, legumes, and whole grains daily not only improves cholesterol but also supports overall heart health.
While fiber supplements are an option, consuming whole foods is always the better choice when possible.
Try The Portfolio Diet
There are also certain foods specifically shown to lower cholesterol. These are included in a dietary pattern called the ‘Portfolio diet’, often used to target high LDL levels. In fact following a Portfolio diet, can potentially lower LDL cholesterol by up to 30 %!! (Jenkins et al., 2003)
Key Portfolio Diet Components
Each day, aim for:
- Soy protein: 50 grams (from sources like tofu, edamame, and miso).
- Plant sterols: 2 grams (found in fortified foods or naturally in small amounts in plants).
- Nuts: 45 grams (about one handful or 23 almonds).
- Soluble fiber: 18 grams (from oats, barley, legumes, and other whole grains).
Each food has an additive effect, so every step you take counts.

How To Lower Triglycerides
While the focus for cholesterol lowering is usually on LDL cholesterol, triglycerides are important too!
High triglycerides are often a marker of insulin resistance, as well as of fatty liver disease and visceral fat, where excess harmful fat is stored in the liver. and internal organs. This fat is highly inflammatory, and if left unaddressed, can progress to more serious conditions.
Fortunately, high triglyceride levels (and visceral fat) are incredibly responsive to simple diet and lifestyle changes!
Here are some effective ways to reduce triglyceride levels and reduce visceral fat and fat in your liver:
- Stay Active: Regular exercise helps burn calories and improves fat metabolism.
- Avoid Overeating: Focus on balanced portions.
- Reduce Simple Carbs: Limit refined carbs, processed foods, and added sugars. This includes liquid sugars like soft drinks and fruit juices!
- Balance Your Plate: Aim for around half your diet to be non starchy veges; 25% to be lean protein (legumes, nuts, seeds, oily fish, chicken or eggs); and 25% to be complex (whole grain) carbohydrates.
- Be Mindful Of Alcohol: Alcohol is both toxic to your liver, and can also significantly increase triglyceride levels. Keep it to a minimum (or avoid it altogether) – ideally aiming for less than 2 standard drinks per week.
Together, these strategies not only lower triglycerides but also reduce the risk of prediabetes, diabetes, and fatty liver disease. Plus they’re great for overall health too!

THE POWER OF THE MEDITTERANEAN DIET
Still Doubting the Impact of Diet? Let’s Dive into the Evidence!
Two of the largest and most groundbreaking studies on diet and heart disease—the LYON Diet Heart Study and the PREDIMED Trial—provide compelling proof that what you eat can significantly affect your heart health.
The LYON Diet Heart Study
This study examined the effects of a Mediterranean-style diet on 500 individuals who had experienced their first heart attack. Participants were divided into two groups:
- Group 1: Continued their standard Western diet.
- Group 2: Adopted a plant-focused Mediterranean diet.
The Mediterranean diet emphasized:
- High intake: Fruits, vegetables, whole grains, potatoes, beans, nuts, and seeds.
- Primary fat source: Olive oil.
- Moderate amounts: Dairy, fish, and poultry.
- Minimal consumption: Eggs (0–4 weekly) and red meat.
Key Results (after 46 months):
- A 60% reduction in overall mortality.
- A 70% reduction in recurrent heart attacks.
The results were so striking that the trial was stopped early. Allowing the control group to continue a Western diet was deemed unethical, given their significantly higher risk of heart attacks and death.
Takeaway: No medication on the market offers such dramatic results as the Mediterranean diet.
The PREDIMED Study
This landmark study followed nearly 7,500 high-risk individuals to assess the impact of diet on heart disease prevention. Participants were divided into three groups:
- A Mediterranean diet supplemented with extra-virgin olive oil.
- A Mediterranean diet supplemented with mixed nuts.
- A standard low-fat diet.
Key Results (after almost 5 years):
- Both Mediterranean diet groups reduced their risk of heart attacks by 30% compared to people who followed a standard low fat diet—a reduction comparable to statin therapy.
Why This Matters
Both studies show that dietary changes alone can produce life-altering benefits for heart health. These results highlight the power of:
- High-fiber, plant-focused eating (as in the Mediterranean diet).
- Healthy fats from olive oil and nuts.
When combined with other heart-healthy habits—such as regular exercise, stress management, adequate sleep, reducing salt intake, and avoiding smoking—the benefits become even more profound.
Conclusion: The evidence is clear—diet is a cornerstone of heart health. It’s never too late to make changes, and the impact can be as significant as, or even greater than, many medications. You can use the graphic below to see how to follow a Mediterranean dietary pattern, like those used in the studies just mentioned.
Even if you’re prescribed statin medications, adopting heart-healthy dietary changes amplifies the benefits. A cholesterol-lowering diet doesn’t just help reduce LDL—it supports overall health and tackles multiple cardiovascular risk factors.
TO WRAP IT ALL UP
So to sum it all up, here are our top tips for improving cholesterol, so you can reduce your risk of heart disease, strokes, dementia, and other health issues:
- Eat whole foods, mostly plants.
- Boost your fiber intake by including fruits, vegetables, legumes, nuts, seeds, and whole grains daily.
- Focus on plant-based cholesterol-lowering foods like oats, soy, legumes, nuts, and plant sterols aka the Portfolio diet.
- Stay active—aim to move your body every day.
- Limit processed foods, added sugars, refined carbs, and alcohol—swap refined grains for whole grains.
- Adopt the Mediterranean diet pattern and use the wellness plate as your guide to balanced eating.
- Reduce saturated fats, especially from animal products, particularly if you have high cholesterol or other cardiovascular risks.
- Embrace anti-inflammatory habits:
- Follow an anti-inflammatory diet.
- Avoid cigarette smoke.
- Limit salt intake.
- Work towards a healthy weight range.
These are the same principles we recommend for overall good health—simple yet incredibly effective!
WANT TO LEARN MORE?
If this resonates with you, we dive deeper into these topics in our Reboot and Nutrition courses, designed to help you transform your health completely.
Need personalized advice? We offer virtual lifestyle medicine consultations across New Zealand (via secure telemedicine) too!. We’d love to work with you to create a tailored, evidence-based plan to optimize your cholesterol, heart health, and overall well-being.
👉 More details here —we can’t wait to help you take control of your health!
References:
Bruckert E, Rosenbaum D. Lowering LDL-cholesterol through diet: potential role in the statin era. Curr Opin Lipidol. 2011 Feb;22(1):43-8. doi: 10.1097/MOL.0b013e328340b8e7. PMID: 21233620.
Gigleux I, Jenkins DJ, Kendall CW, et al. Comparison of a dietary portfolio diet of cholesterol-lowering foods and a statin on LDL particle size phenotype in hypercholesterolaemic participants. Br J Nutr. 2007 Dec;98(6):1229-36. doi: 10.1017/S0007114507781461. Epub 2007 Jul 30. PMID: 17663803.
Bitzur R, Cohen H, Kamari Y, Harats D. [Phytosterols: another way to reduce LDL cholesterol levels]. Harefuah. 2013 Dec;152(12):729-31, 751. Hebrew. PMID: 24482998.
Ras RT, Geleijnse JM, Trautwein EA. LDL-cholesterol-lowering effect of plant sterols and stanols across different dose ranges: a meta-analysis of randomised controlled studies. Br J Nutr. 2014 Jul 28;112(2):214-9. doi: 10.1017/S0007114514000750. Epub 2014 Apr 29. PMID: 24780090; PMCID: PMC4071994.
Anderson KM, Castelli WP, Levy D. Cholesterol and mortality. 30 years of follow-up from the Framingham study. JAMA. 1987 Apr 24;257(16):2176-80. doi: 10.1001/jama.257.16.2176. PMID: 3560398.
Anderson, T. J., Gregoire, J., Pearson, G. J., Barry, A. R., et al. (2016). 2016 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in the Adult. Can J Cardiol, 32(11), 1263-1282.
Asbaghi, O., Moodi, V., Hadi, A., Eslampour, E., Shirinbakhshmasoleh, M., et al. (2021). The effect of almond intake on lipid profile: a systematic review and meta-analysis of randomized controlled trials. Food Funct, 12(5), 1882-1896.
Basora, J., Munoz, M. A., Sorli, J. V., Martinez, J. A., Fito, M., Gea, A., . . . Investigators, P. S. (2018). Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N Engl J Med, 378(25), e34.
Blanco Mejia, S., Messina, M., Li, S. S., Viguiliouk, E., Chiavaroli, L., Khan, T. A., et al. (2019). A Meta-Analysis of 46 Studies Identified by the FDA Demonstrates that Soy Protein Decreases Circulating LDL and Total Cholesterol Concentrations in Adults. J Nutr, 149(6), 968-981.
Chiavaroli, L., Nishi, S. K., Khan, T. A., Braunstein, C. R et al (2018). Portfolio Dietary Pattern and Cardiovascular Disease: A Systematic Review and Meta-analysis of Controlled Trials. Prog Cardiovasc Dis,61(1), 43-53.
Chiavaroli, L., Viguiliouk, E., Nishi, S. K., Blanco Mejia, S., Rahelic, D et al. (2019). DASH Dietary Pattern and Cardiometabolic Outcomes: An Umbrella Review of Systematic Reviews and Meta-Analyses. Nutrients, 11(2).
de Souza, R. J., Mente, A., Maroleanu, A., Cozma, A. I., Ha, V., Kishibe, T., Uleryk, E., Budylowski, P., Schünemann, H., Beyene, J., & Anand, S. S. (2015). Intake of saturated and trans unsaturated fatty acids and risk of all cause mortality, cardiovascular disease, and type 2 diabetes: systematic review and meta-analysis of observational studies. BMJ (Clinical research ed.), 351, h3978.
Estruch, R., Ros, E., Salas-Salvado, J., Covas, M. I., Corella, D., Aros, F., Gomez-Gracia, E., Ruiz-Gutierrez, V., et sl(2016a). The effect of oat beta-glucan on LDL-cholesterol, non-HDL-cholesterol and apoB for CVD risk reduction: a systematic review and meta-analysis of randomised-controlled trials. Br J Nutr, 116(8), 1369-1382.
Ho, H. V., Sievenpiper, J. L., Zurbau, A., Blanco Mejia, S., Jovanovski, E., Au-Yeung, F., Jenkins, A. L., & Vuksan, V. (2016b). A systematic review and meta-analysis of randomized controlled trials of the effect of barley beta-glucan on LDL-C, non-HDL-C and apoB for cardiovascular disease risk reduction(i-iv). Eur J Clin Nutr,70(11), 1239-1245.
Hooper, L., Martin, N., Jimoh, O. F., Kirk, C., Foster, E., & Abdelhamid, A. S. (2020). Reduction in saturated fat intake for cardiovascular disease. The Cochrane database of systematic reviews, 5(5), CD011737.
Jenkins D, et al. Effects of a dietary portfolio of cholesterol-lowering foods vs lovastatin on serum lipids and C-reactive protein. JAMA. 2003 Jul 23;290(4):502-10. doi: 10.1001/jama.290.4.502.
Martinez-Gonzalez, M. A., Gea, A., & Ruiz-Canela, M. (2019). The Mediterranean Diet and Cardiovascular Health. Circ Res, 124(5), 779-798.
Mazidi, M., Mikhailidis, D. P., Sattar, N., Toth, P. P., Judd, S., Blaha, M. J., Hernandez, A. V., Penson, P. E., Banach, M., & International Lipid Expert Panel (ILEP) & Lipid and Blood Pressure Meta-analysis Collaboration (LBPMC) Group (2020). Association of types of dietary fats and all-cause and cause-specific mortality: A prospective cohort study and meta-analysis of prospective studies with 1,164,029 participants. Clinical nutrition (Edinburgh, Scotland), 39(12), 3677–3686.
Pearson, G. J., Thanassoulis, G., Anderson, T. J., Barry, A. R., Couture, P., Dayan, N., Francis, G. A., et al(2021). 2021 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in Adults. Can J Cardiol, 37(8), 1129-1150.
Quek, J., Lim, G., Lim, W. H., Ng, C. H., So, W. Z., Toh, J., Pan, X. H., Chin, Y. H., Muthiah, et al. (2021). The Association of Plant-Based Diet With Cardiovascular Disease and Mortality: A Meta-Analysis and Systematic Review of Prospect Cohort Studies. Front Cardiovasc Med, 8, 756810.
Schoeneck, M., & Iggman, D. (2021). The effects of foods on LDL cholesterol levels: A systematic review of the accumulated evidence from systematic reviews and meta-analyses of randomized controlled trials. Nutrition, metabolism, and cardiovascular diseases : NMCD, 31(5), 1325–1338.
Tokede, O. A., Onabanjo, T. A., Yansane, A., Gaziano, J. M., & Djousse, L. (2015). Soya products and serum lipids: a meta-analysis of randomised controlled trials. Br J Nutr, 114(6), 831-843.
Trautwein, E. A., Vermeer, M. A., Hiemstra, H., & Ras, R. T. (2018). LDL-Cholesterol Lowering of Plant Sterols and Stanols-Which Factors Infl
uence Their Efficacy? Nutrients, 10(9).
Vincent, M. J., Allen, B., Palacios, O. M., Haber, L. T., & Maki, K. C. (2019). Meta-regression analysis of the effects of dietary cholesterol intake on LDL and HDL cholesterol. The American journal of clinical nutrition, 109(1), 7–16.
Zhuang, P., Wu, F., Mao, L., Zhu, F., Zhang, Y., Chen, X., Jiao, J., & Zhang, Y. (2021). Egg and cholesterol consumption and mortality from cardiovascular and different causes in the United States: A population-based cohort study. PLoS medicine, 18(2), e1003508.
Bittner V, Johnson BD, Zineh I, Rogers WJ, Vido D, Marroquin OC, Bairey-Merz CN, Sopko G. The triglyceride/high-density lipoprotein cholesterol ratio predicts all-cause mortality in women with suspected myocardial ischemia: a report from the Women’s Ischemia Syndrome Evaluation (WISE). Am Heart J. 2009 Mar;157(3):548-55. doi: 10.1016/j.ahj.2008.11.014. PMID: 19249427; PMCID: PMC2677623.
Summary of evidence for lifestyle strategies to reduce cholesterol
https://academic.oup.com/eurheartj/article/41/1/111/5556353?login=false (European lipid guidelines)



{kind=link}